Administration of Dosages
The dosage amount varies by the Estradiol Ester you use (EV, EEn, etc) and how you administer it. Here’s a table of approximate doses: https://transfemscience.org/articles/e2-equivalent-doses/
Doses should be divided in equal parts in the day. Divide 24 (hours in the day) by number of pills you will be taking. For instance, for 2 pills (4 mg), take them 12 hours apart. For 3 (6 mg), 8 hours apart, and so on.
4 mg daily is the usual recommended dose, paired with an Anti-Androgen.
Monotherapy on pills often does not work due to the instability in levels received from them. Those who do take it usually require 6 mg to 8 mg when on Estradiol Valerate pills. Taking them sublingually and at consistent times is effectively necessary if you go down this route.
The two main ways to administer these pills are:
Oral
The pills are swallowed and absorbed through the digestive tract. It passes through the liver first (first pass metabolism), which might increase liver protein production and could increase the risk of blood clots. It shouldn’t be a problem if you have a healthy liver and no family history of bad livers. This gives you more stable estrogen levels than if you were to take it sublingually. However, absorption is less efficient than sublingual, meaning you receive lower E levels on the same dose.
Sublingual
The pill is placed under the tongue, and gets absorbed directly into the blood stream. Liver related risks are thus very low to non. It also gives higher levels in the blood. However, the peaks are highwith a quicker onset, but also subside faster, which may result in unstable levels. This makes dividing the dose equally over the day more important.
The dosage amount varies by the Estradiol Ester you use (EV, EEn, etc) and how you administer it. Here’s a table of approximate doses: https://transfemscience.org/articles/e2-equivalent-doses/
Monotherapy on EEn injectables is quite easy, and is the recommended form of HRT. Usual doses for this are 5 mg every 7 days, or 7 mg every 10 days.
You can run some simulations of potential doses, taking into account the specific formulation you’ll be taking, on the Estradiol Pharmacokinetics Playground. Keep in mind that these are estimates and do not take your specific body into account.
In some cases, monotherapy does not provide sufficient T suppression, especially in initial period. In such cases, taking a low dosage of an AA alongside the injecition dose may be considered. AA dosage will vary by your T levels while on monotherapy.
For a guide on how to inject yourself, check out the Self Injection Guide
Refer to the DIY HRT wiki. All three options mentioned must be taken orally.
Dosage and how they should be divided over the day varies by T suppression required, the type of AA you take, and how your body reacts to it. Here’s a chart showing a rough working:
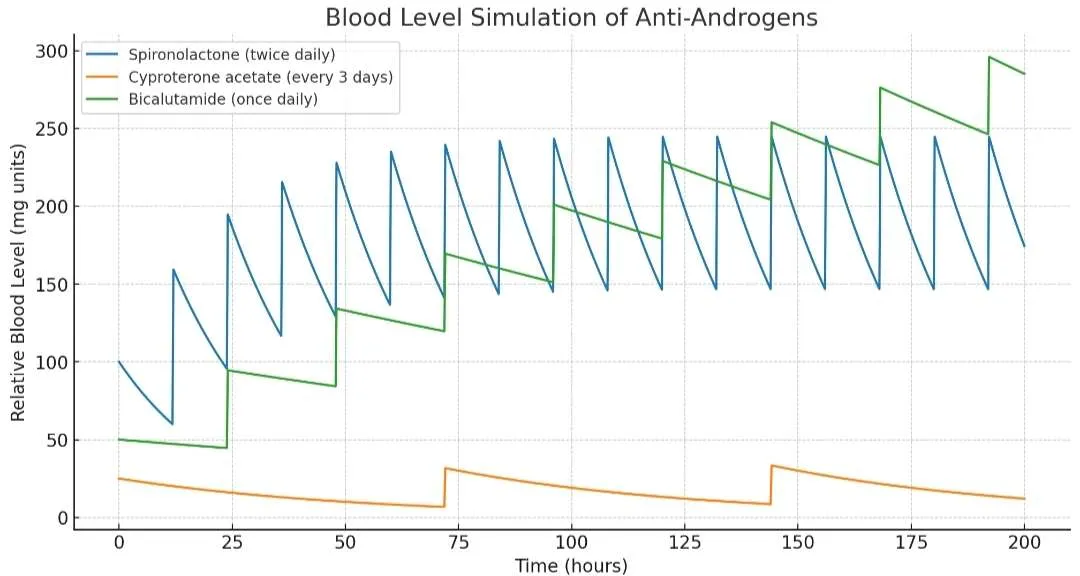
As seen in the chart, the half-lives of each of the options vary significantly. As such, a general recommendation in combination with 4 mg E pills would be one of:
- 12.5 mg CPA daily, though this can be moved to every other day after the initial period.
- 50 mg Spiro twice a day (100 mg total)
- 50 mg Bicalutamide daily
This CPA dosage, of course, means the CPA you receive from Climen is not sufficient, and Androcur is a necessary purchase if you choose it as your Anti-Androgen. If you do take the pink tablets from Climen in addition to Androcur, make sure your total CPA dose does not exceed 12.5 mg a day.
Consider taking CPA before bedtime, as it can induce sleepiness.
Dosage should usually be 200 mg daily, though it can be increased to 400 mg if you take it orally.
The two main ways of administering these are:
Oral
The capsule is swallowed, and it gets absorbed through the gut. Due to first-pass metabolism in the liver, producing metabolites like allopregnanolone, which can cause alcohol-like side effects including more sedation or drowsiness. Compared to taking them rectally, the bioavailability is lower as the dose is broken down before reaching circulation, resulting in lower levels of progesterone.
Rectal
Capsule is inserted into the rectum and absorbed. It partially bypasses first-pass metabolism, giving higher blood levels from the same dose. This method often causes less sedation, but can still have systemic effects.
Oral capsules can be taken rectally too, and it is the preferred route.